Table of Contents
1. Definition
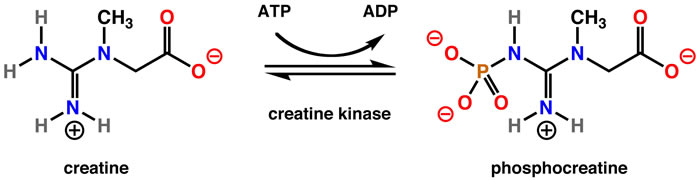
Creatine kinase (CK), also called creatine phosphokinase (CPK), is an intracellular enzyme that catalyzes the reversible conversion:Creatine+ATP↔Phosphocreatine+ADPCreatine + ATP \leftrightarrow Phosphocreatine + ADPCreatine+ATP↔Phosphocreatine+ADP
This reaction is crucial for energy storage and rapid regeneration of ATP, especially in muscle and brain tissues.
2. Location in Body
CK is present mainly in tissues with high energy demand:
| Tissue | CK concentration |
|---|---|
| Skeletal muscle | Highest |
| Cardiac muscle | High |
| Brain | Moderate |
| Smooth muscle | Low |
Because CK is intracellular, serum CK rises when cell membrane damage occurs.
3. CK Isoenzymes
CK exists in three isoenzymes, formed by combinations of M (muscle) and B (brain) subunits.
| Isoenzyme | Structure | Major Source | Clinical significance |
|---|---|---|---|
| CK-MM | M + M | Skeletal muscle | Muscle injury, rhabdomyolysis |
| CK-MB | M + B | Cardiac muscle | Myocardial injury |
| CK-BB | B + B | Brain, smooth muscle | CNS injury |
Distribution
- CK-MM: ~95–100% of total CK in normal serum
- CK-MB: <5% normally
- CK-BB: normally absent in serum
4. Normal Values
Normal ranges vary by lab.
Typical reference:
| Group | CK (U/L) |
|---|---|
| Adult male | 50–200 |
| Adult female | 40–150 |
| Children | Higher than adults |
| Neonates | Can be very high after birth |
5. Causes of Elevated CK

A. Skeletal Muscle Disorders
Most common cause.
Examples:
- Muscular dystrophy (e.g., Duchenne muscular dystrophy)
- Inflammatory myopathies
- Polymyositis
- Dermatomyositis
- Trauma
- Intramuscular injections
- Vigorous exercise
B. Rhabdomyolysis
Massive CK elevation.
Causes:
- Crush injury
- Drugs (statins)
- Heat stroke
- Severe infections
CK may rise >5000–10,000 U/L.

C. Cardiac Causes
CK-MB rises in myocardial injury.
Example:
- Myocardial Infarction
However, CK-MB is now largely replaced by troponins.
D. Neurologic Disorders
CK-BB may increase in:
- Stroke
- Brain trauma
- Seizures
Example:
- Stroke
E. Other Causes
- Hypothyroidism
- Alcohol abuse
- Surgery
- Prolonged immobilization
- Severe infections
6. CK in Myocardial Infarction
Historically important marker.
| Parameter | CK-MB |
|---|---|
| Rise | 3–6 hours |
| Peak | 12–24 hours |
| Normalization | 48–72 hours |
Used previously to detect reinfarction.
Now replaced mainly by troponin I/T.
7. CK in Pediatric Practice
Important uses:
Screening for muscular dystrophy
Very high CK in:
- Duchenne muscular dystrophy
- Becker muscular dystrophy
Levels may be 10–100× normal.
Evaluation of Hypotonia
Used when evaluating:
- floppy infant
- muscle weakness
Evaluation of Rhabdomyolysis
Symptoms:
- myalgia
- weakness
- dark urine (myoglobinuria)
8. Causes of Decreased CK
Rare clinical significance.
Seen in:
- Low muscle mass
- Chronic illness
- Pregnancy
9. Drugs Causing Elevated CK
Important clinically.
Examples:
| Drug | Mechanism |
|---|---|
| Statins | Myopathy |
| Antipsychotics | Neuroleptic malignant syndrome |
| Corticosteroids | Muscle breakdown |
Example condition:
Neuroleptic Malignant Syndrome
10. Investigation Panel When CK is Elevated
| Test | Purpose |
|---|---|
| CK-MB | Cardiac source |
| Troponin | MI confirmation |
| AST / ALT | Muscle vs liver |
| LDH | Tissue injury |
| Serum myoglobin | Rhabdomyolysis |
| Urine myoglobin | Kidney injury |
11. CK in Rhabdomyolysis Severity
| CK level | Interpretation |
|---|---|
| <1000 | Mild |
| 1000–5000 | Moderate |
5000 | Severe muscle injury |
15000 | High risk of renal failure |
12. Clinical Pearls (Exam High-Yield)
- CK-MM → skeletal muscle injury
- CK-MB → cardiac muscle
- CK-BB → brain
- Duchenne muscular dystrophy → CK extremely high
- CK rises after muscle trauma/exercise
- CK-MB replaced by troponin in MI diagnosis
✅ One-line exam memory tip
“CK rises with muscle damage — skeletal (MM), cardiac (MB), brain (BB).”