Table of Contents
A cesarean section, commonly called a C-section, is a surgical procedure used to deliver a baby through incisions made in the mother’s abdomen and uterus. It may be planned in advance or performed as an emergency procedure when vaginal delivery could pose risks to the mother or baby.
C-sections are common worldwide and can be life-saving. However, because they involve major abdominal surgery, recovery usually takes longer than recovery after a vaginal birth. Understanding the healing process and following proper post-operative care can help mothers recover more comfortably and reduce the risk of complications.
What Happens During a Cesarean Section?
During a C-section, doctors make an incision through the abdominal wall and uterus to safely deliver the baby. The procedure is typically performed under spinal or epidural anesthesia, allowing the mother to remain awake while avoiding pain.
Common reasons for a cesarean delivery include:
- Prolonged or difficult labor
- Fetal distress
- Multiple pregnancies (twins or more)
- Breech position
- Placenta-related complications
- Previous cesarean delivery
- Certain maternal health conditions

Healing Time After a C-Section
Recovery varies from person to person, but most women follow a general healing timeline.
First 24–48 Hours
- Mothers are closely monitored in the hospital.
- Pain, fatigue, and abdominal soreness are common.
- Walking is encouraged within a day to improve circulation and prevent blood clots.
First 2 Weeks
- Incision pain gradually decreases.
- Light movement becomes easier.
- Bleeding and discharge may continue.
- Rest is essential.
4–6 Weeks
- Most tissues heal significantly during this period.
- Many women can return to light household activities.
- Driving and moderate activity may resume after medical approval.
6–12 Weeks
- Internal healing continues.
- Energy levels improve.
- Exercise can slowly restart with a doctor’s guidance.
Even after the external scar appears healed, internal tissues may still be recovering. Full recovery can sometimes take several months.
Common Symptoms During Recovery
The following symptoms are usually normal after a C-section:
- Mild to moderate incision pain
- Cramping
- Vaginal bleeding
- Fatigue
- Swelling
- Difficulty standing fully upright initially
- Temporary numbness around the incision
However, worsening symptoms should never be ignored.
Tips for Faster Recovery
1. Get Adequate Rest
Sleep and rest are essential for tissue repair and hormonal recovery. New mothers should rest whenever the baby sleeps and avoid overexertion.
2. Walk Regularly
Gentle walking improves blood circulation, reduces gas pain, and lowers the risk of blood clots. Short walks several times daily are beneficial.
3. Support the Incision
Holding a pillow against the abdomen while coughing, laughing, or standing can reduce discomfort and protect the incision.
4. Stay Hydrated
Drinking enough water supports healing, digestion, and breast milk production.
5. Eat Nutritious Foods
A balanced diet rich in protein, iron, vitamins, and fiber helps tissue repair and prevents constipation.
Helpful foods include:
- Lean meats and eggs
- Fruits and vegetables
- Whole grains
- Yogurt
- Nuts and seeds
6. Avoid Heavy Lifting
For at least 6 weeks, mothers should avoid lifting anything heavier than the baby.
7. Take Medications as Prescribed
Pain medicines and antibiotics should be taken exactly as directed.
8. Keep the Incision Clean and Dry
Gentle cleaning and proper drying reduce infection risk. Tight clothing should be avoided if it irritates the wound.
9. Accept Help From Others
Support from family members can reduce physical strain and emotional stress during recovery.
10. Attend Follow-Up Appointments
Regular medical checkups help ensure proper healing and early detection of complications.
Preventing Complications
While most women recover well, complications can occur if proper care is neglected.
Preventing Infection
Signs of infection include:
- Redness
- Swelling
- Fever
- Pus or foul-smelling discharge
- Increasing pain
To prevent infection:
- Wash hands before touching the incision.
- Follow wound-care instructions carefully.
- Avoid soaking in bathtubs until approved by a doctor.
Preventing Blood Clots
After surgery, blood clot risk increases temporarily.
Prevention measures include:
- Early walking
- Leg exercises
- Staying hydrated
- Wearing compression stockings if recommended
Preventing Constipation
Pain medications and reduced movement may slow digestion.
Helpful strategies:
- Drink water
- Eat fiber-rich foods
- Walk regularly
- Use stool softeners if prescribed
Emotional Health Matters
Some mothers experience anxiety, sadness, or emotional overwhelm after delivery.
Seek medical support if symptoms include:
- Persistent sadness
- Loss of interest
- Severe mood swings
- Difficulty bonding with the baby
- Thoughts of self-harm
Postpartum depression is treatable and should never be ignored.
When to Seek Immediate Medical Care
A doctor should be contacted immediately if any of the following occur:
- High fever
- Heavy bleeding
- Severe abdominal pain
- Chest pain or breathing difficulty
- Swelling or pain in one leg
- Opening of the incision
- Foul-smelling wound drainage
- Persistent vomiting
These symptoms may indicate serious complications that require urgent treatment.
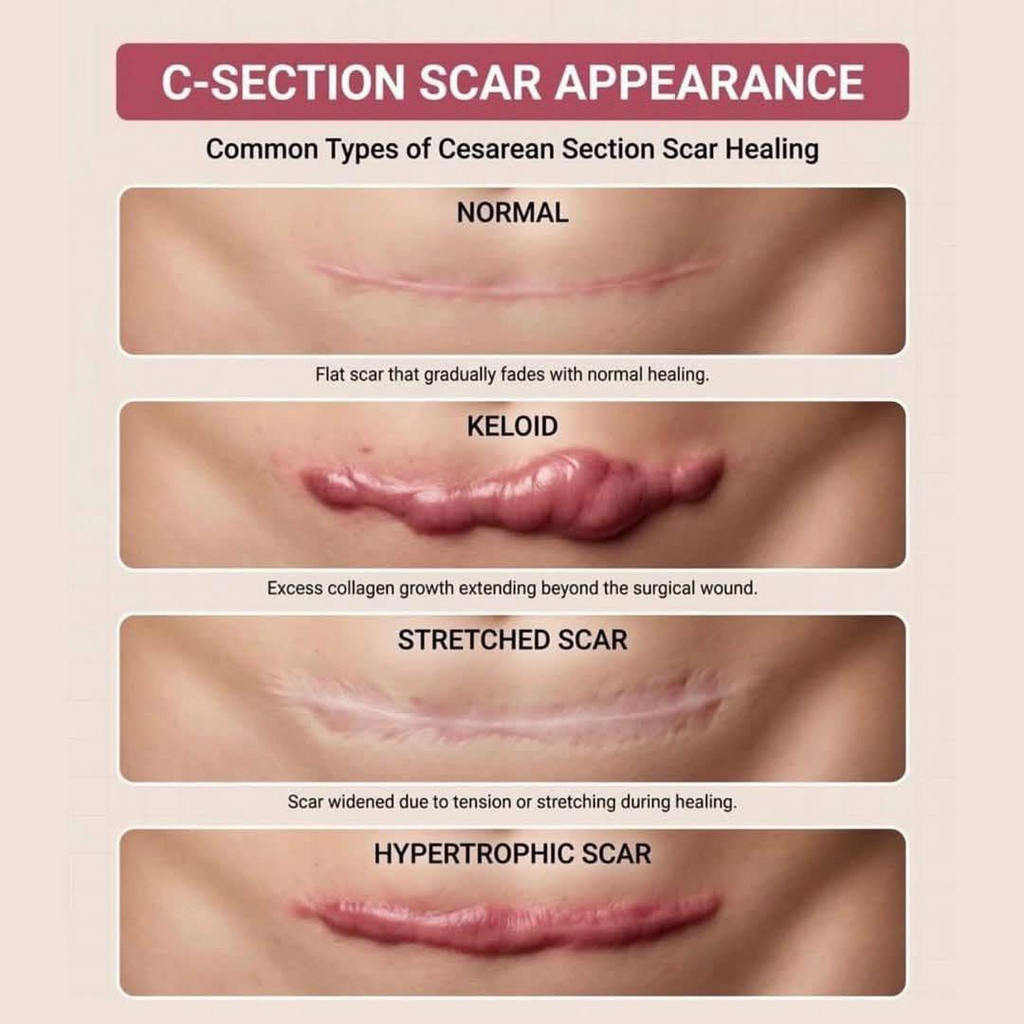
Long-Term Recovery and Scar Healing
C-section scars usually fade gradually over time. Gentle scar care after complete wound closure may improve appearance.
Long-term recovery tips include:
- Gradually rebuilding core strength
- Maintaining a healthy weight
- Avoiding smoking
- Discussing future pregnancy plans with a healthcare provider
Many women go on to have healthy future pregnancies and deliveries after a cesarean section.
Conclusion
A cesarean section is a major surgical procedure that requires patience, rest, and proper care during recovery. Most mothers heal well within several weeks, especially when they follow healthy recovery habits and seek medical help promptly when needed.
Good nutrition, gentle movement, incision care, emotional support, and regular medical follow-up all play important roles in faster healing and complication prevention. With appropriate care and support, mothers can recover safely while focusing on bonding with their newborn and adjusting to life after childbirth.