
Table of Contents
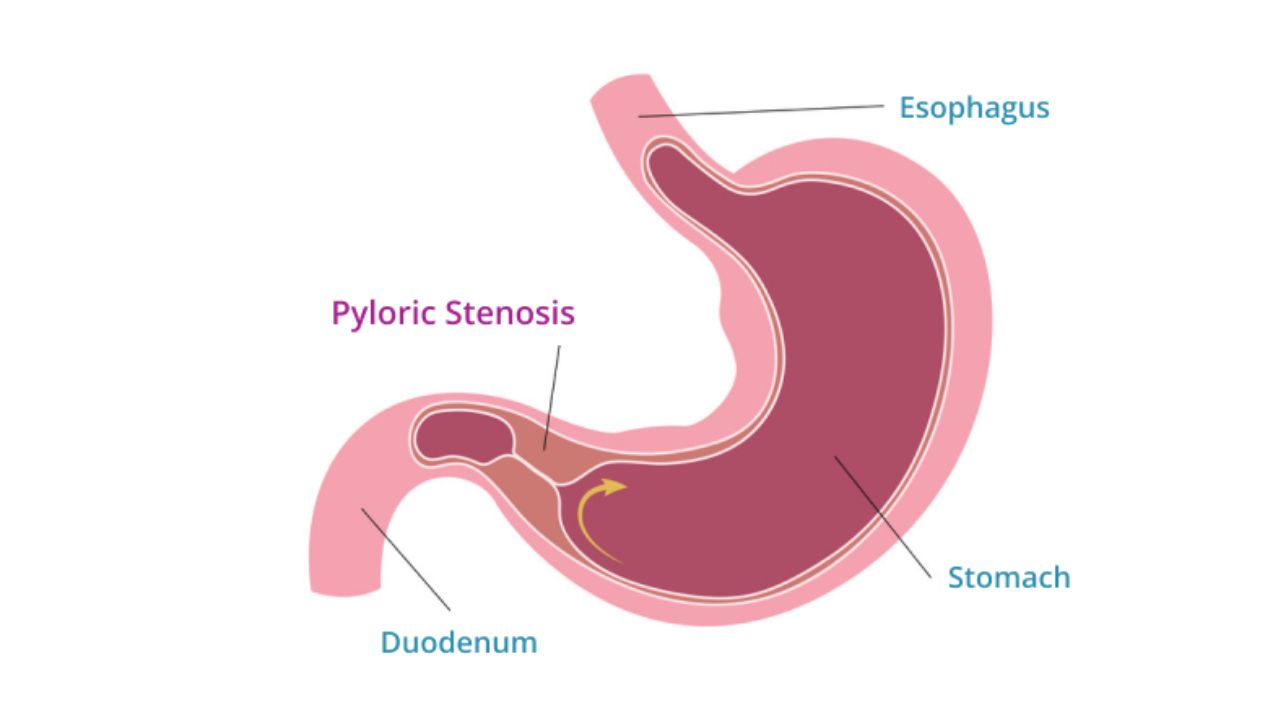
Definition
- Hypertrophy + hyperplasia of pyloric muscle → gastric outlet obstruction in infants.
Epidemiology
- Age: 2–8 weeks (classically 3–6 weeks)
- More common in:
- First-born males
- Formula-fed infants
- Positive family history
- Associated with macrolide exposure (e.g., erythromycin)
Pathology
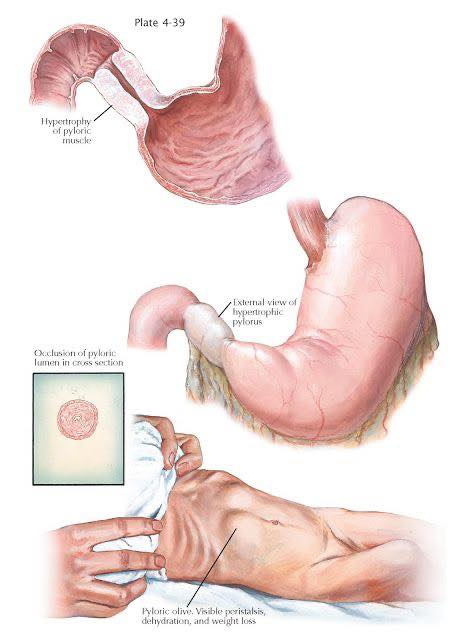
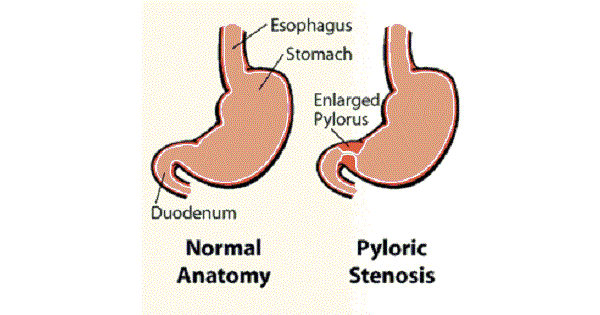
- Thickened pyloric muscle narrows pyloric canal.
- Causes obstruction to gastric emptying.
Clinical Features
Classic Triad
- Projectile non-bilious vomiting
- Visible gastric peristalsis
- Olive-shaped mass in epigastrium/right upper abdomen

Other Findings
- Hungry after vomiting (“hungry vomiter”)
- Weight loss/dehydration
- Constipation
- Failure to thrive
Why Vomiting is Non-Bilious?
- Obstruction is proximal to duodenum → bile cannot enter vomitus.

Electrolyte Abnormality (Very Important)
Due to repeated vomiting:
- Hypochloremic
- Hypokalemic
- Metabolic alkalosis
Mnemonic:
“Vomiting loses HCl”
Diagnosis
Investigation of Choice
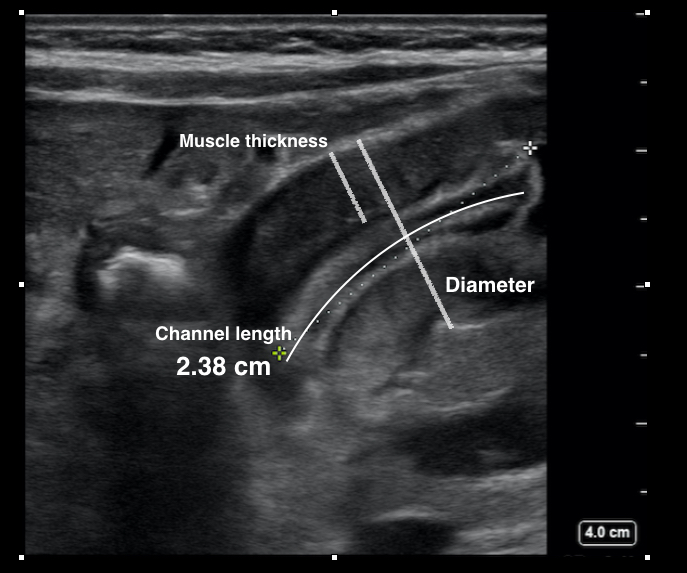
- Ultrasound abdomen
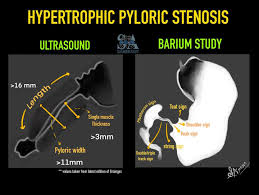
USG Findings
- Thickened pylorus
- Elongated pyloric canal

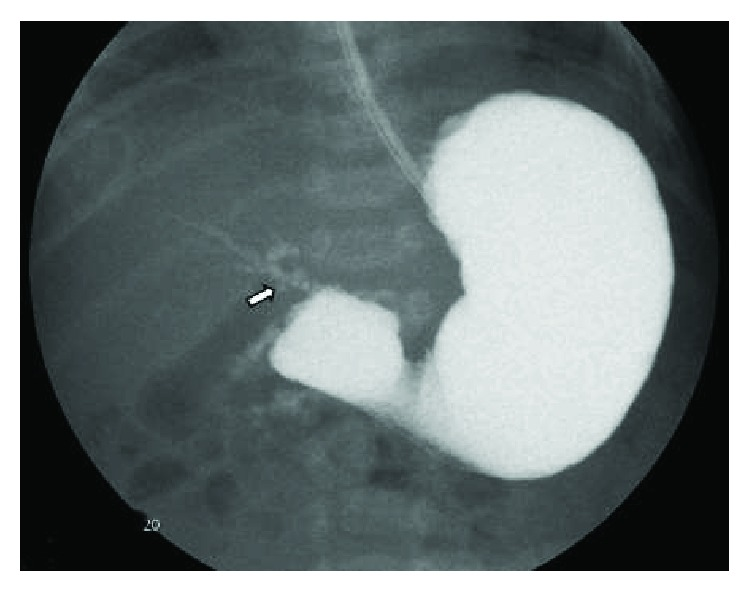
X-ray/Barium
- “String sign” (narrowed pyloric canal)

Management
Initial
- Correct:
- Dehydration
- Electrolyte imbalance
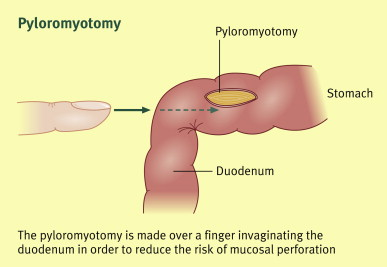
Definitive Treatment
- Ramstedt pyloromyotomy

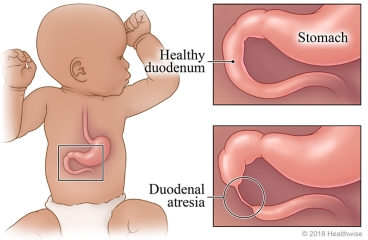
Important Differentials
- Gastroesophageal reflux
- Duodenal atresia (bilious vomiting)
- Intestinal obstruction
- Sepsis/metabolic disorders

Super High-Yield One-Liners
- Projectile non-bilious vomiting in a 3-week-old male = HPS until proven otherwise
- Olive mass + visible peristalsis = classic clue
- Best diagnostic test = Ultrasound
- Treatment = Pyloromyotomy
- Metabolic alkalosis is the classic acid-base disorder

Quick Revision Table
| Feature | HPS |
|---|---|
| Age | 2–8 weeks |
| Vomiting | Projectile, non-bilious |
| Appetite | Hungry after vomiting |
| Mass | Olive-shaped |
| Diagnosis | Ultrasound |
| Electrolytes | Hypochloremic hypokalemic metabolic alkalosis |
| Treatment | Ramstedt pyloromyotomy |