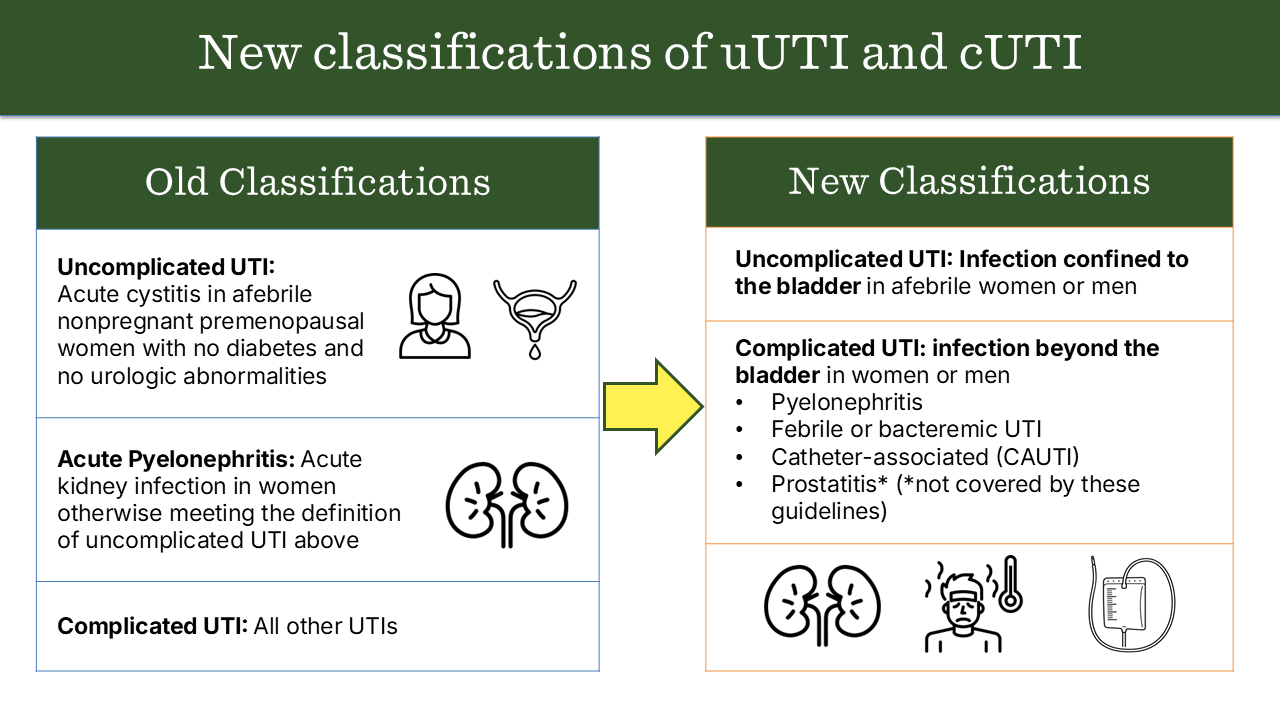
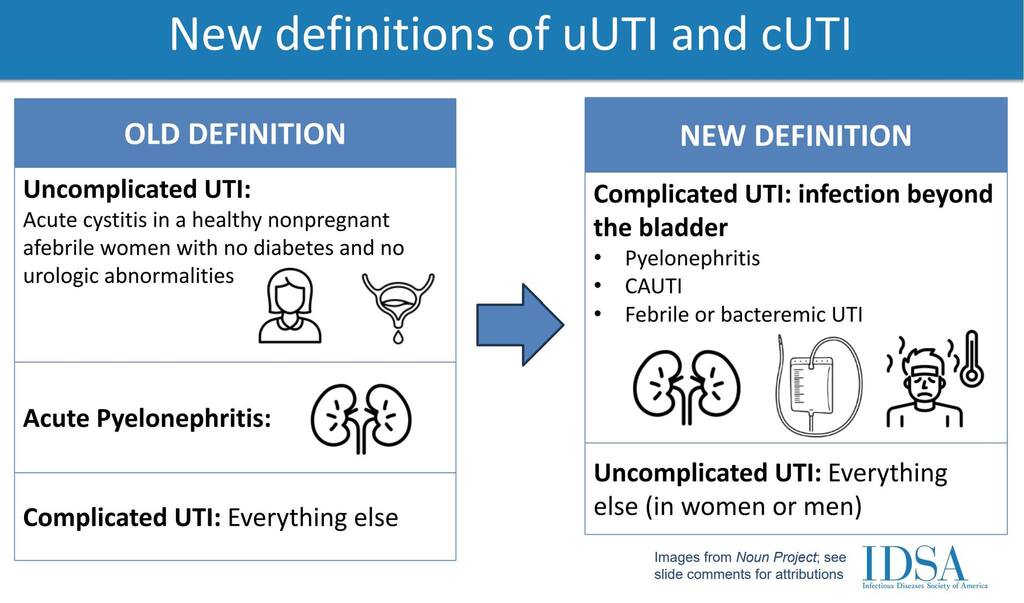
Infection of the lower urinary tract (bladder and urethra) occurring in an otherwise healthy, non-pregnant woman with a structurally and functionally normal urinary tract.
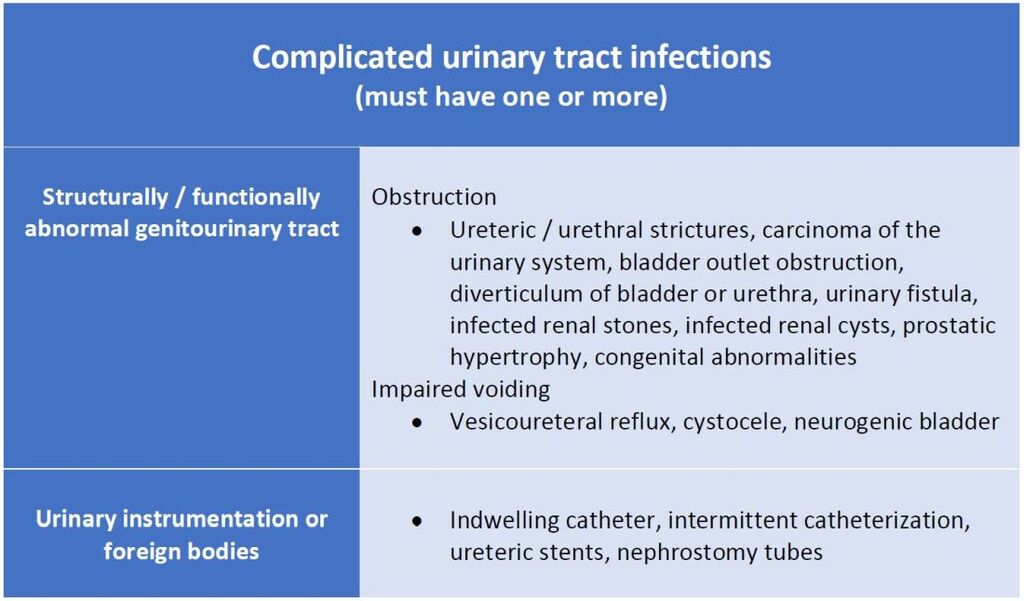
Complicated UTI
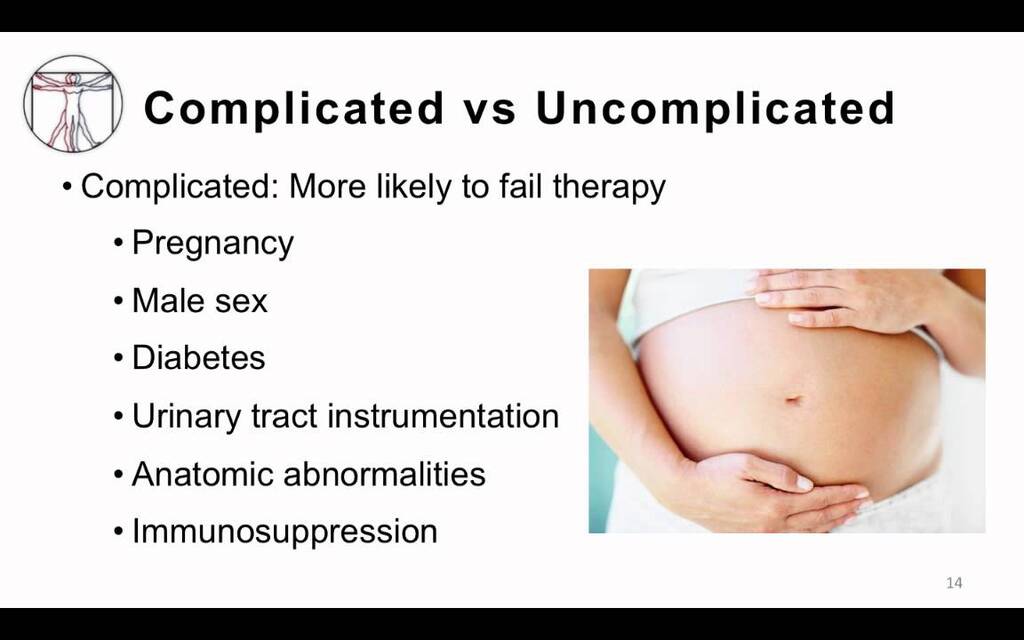
UTI occurring in individuals with structural or functional abnormalities of the urinary tract, comorbidities, or other risk factors that increase risk of treatment failure or recurrence.
Longer course (7–14 days), guided by culture; IV therapy if severe (Ceftriaxone, Piperacillin-tazobactam, Carbapenems for MDR); treat underlying cause (remove catheter, relieve obstruction)
8. Prognosis
Type
Prognosis
Uncomplicated
Excellent, low recurrence with proper hygiene
Complicated
Risk of recurrence, sepsis, renal scarring, abscess