Doxycycline is a broad-spectrum, semisynthetic tetracycline antibiotic that inhibits bacterial protein synthesis by binding to the 30S ribosomal subunit. It is bacteriostatic and effective against gram-positive, gram-negative, and atypical organisms.
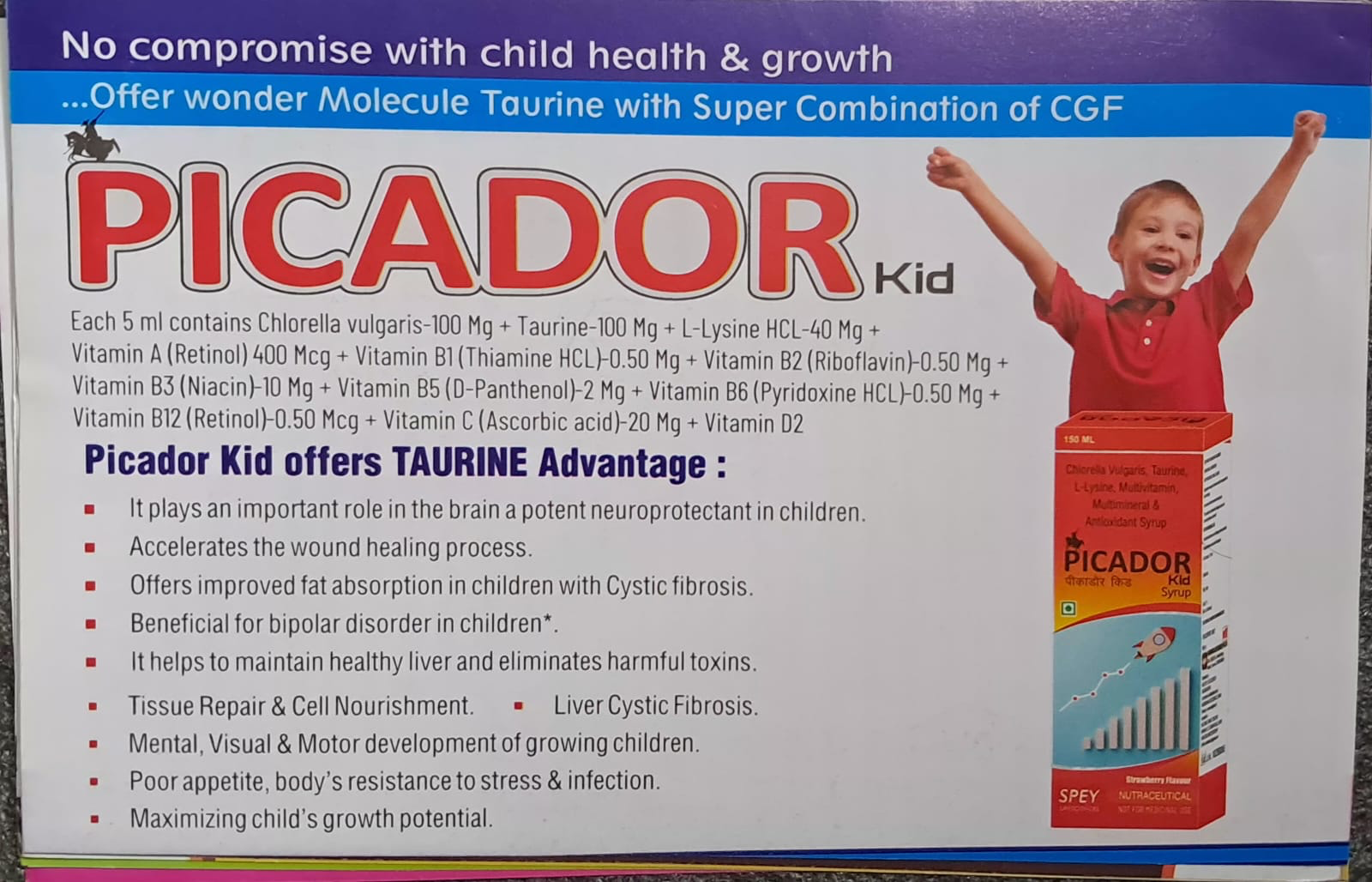
In today’s fast-paced world, ensuring optimal growth and development in children can be challenging, but PICADOR Kid Syrup is here. Nutritional gaps, poor appetite, and frequent infections often compromise a child’s full potential. Picador Kid Syrup is a thoughtfully formulated pediatric supplement designed to support brain development, immunity, and overall growth.
🧪 What Makes Picador Kid Unique?
Each 5 ml of Picador Kid contains a powerful blend of essential nutrients:
Chlorella vulgaris (100 mg) – Rich in proteins and antioxidants
Taurine (100 mg) – A key amino acid for brain and eye development
L-Lysine HCl (40 mg) – Supports growth and appetite stimulation
Vitamin A (400 mcg) – Essential for vision and immunity
Vitamin B Complex (B1, B2, B3, B5, B6, B12) – Boosts metabolism and energy
Vitamin C (20 mg) – Enhances immunity and healing
Vitamin D2 – Supports bone health
This balanced combination ensures comprehensive nutritional support for growing children.
🧠 The Taurine Advantage
One of the standout components of Picador Kid is Taurine, often referred to as a “wonder molecule” in pediatric nutrition.
Key benefits of Taurine:
Acts as a neuroprotectant, supporting brain development
Helps in visual and motor development
Enhances fat absorption, especially beneficial in conditions like cystic fibrosis
Supports liver health and detoxification
Plays a role in tissue repair and cellular nourishment
🌱 Benefits for Growing Children
Picador Kid syrup offers multiple advantages:
✔️ Supports Brain & Cognitive Development
Taurine and B vitamins work together to enhance neurological growth and cognitive function.
✔️ Boosts Immunity
With Vitamin C, Vitamin A, and antioxidants, it strengthens resistance against infections.
✔️ Improves Appetite
L-Lysine helps stimulate appetite in children with poor eating habits.
✔️ Enhances Growth Potential
Provides essential nutrients required for physical growth and development.
✔️ Aids Recovery & Healing
Supports faster wound healing and tissue repair.
✔️ Promotes Liver Health
Helps maintain a healthy liver and assists in toxin elimination.
🧒 Who Can Benefit?
Picador Kid is especially useful for:
Children with poor appetite
Kids with frequent infections
Those with growth delays
Children recovering from illness
Cases requiring nutritional supplementation
⚠️ Important Considerations
While Picador Kid offers multiple benefits, it should be used under medical guidance, especially in:
Children with chronic illnesses
Suspected metabolic or liver disorders
Long-term supplementation needs
Claims like benefits in bipolar disorder or cystic fibrosis should be interpreted cautiously and require evidence-based clinical context.
📝 Final Thoughts
Picador Kid Syrup combines modern nutritional science with essential micronutrients to support holistic child development. Its taurine-rich formulation, along with vitamins and amino acids, makes it a promising supplement for improving appetite, immunity, and growth.
However, like all supplements, it should complement—not replace—a balanced diet, proper sleep, and healthy lifestyle.
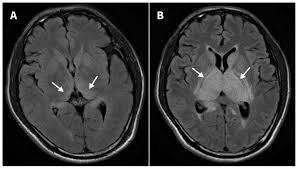
For Japanese Encephalitis (JE), CT findings are not always very sensitive early on, but there are classical (almost pathognomonic) patterns you should remember:
Key Pathognomonic CT Finding
👉 Bilateral thalamic hypodensities
Most characteristic feature
Typically bilateral, symmetrical low-density lesions
May show hemorrhagic changes in severe cases
Other Supporting CT Findings
(Not strictly pathognomonic but highly suggestive in right clinical setting)
Basal ganglia involvement
Midbrain involvement
Brainstem lesions
Cerebellar involvement (less common)
Diffuse cerebral edema in severe cases
Important Clinical Correlation
JE has a predilection for deep gray matter, especially thalamus
For decades, climbing Mount Everest has symbolized human endurance, ambition, and adventure. But beneath the icy peaks and heroic summits, a disturbing reality has emerged—one that threatens not only climbers’ safety but also the integrity of Nepal’s tourism industry.
Recent investigations have exposed a multi-million-dollar insurance fraud scheme centered around unnecessary—and sometimes deliberately staged—helicopter rescues in the Everest region.
What Is the Everest Rescue Insurance Fraud?
The Everest rescue insurance fraud refers to a coordinated system in which trekking guides, helicopter companies, hospitals, and agents allegedly collaborate to generate false or exaggerated medical emergencies. These fake emergencies trigger costly helicopter evacuations, which are then billed to international insurance companies.
Between 2022 and 2025:
Over 300 suspicious rescues were identified (www.ndtv.com)
Fraudulent claims reached nearly $20 million (www.ndtv.com)
Thousands of climbers may have been affected (People.com)
This is not a small scam—it is a systemic exploitation of high-altitude rescue systems.
How the Scam Works
The fraud relies on the unique environment of the Himalayas, where medical uncertainty and remoteness create opportunities for manipulation.
Typical Pattern:
A trekker develops mild symptoms (headache, fatigue, nausea).
A guide exaggerates the risk of acute mountain sickness.
The trekker is pressured into evacuation “for safety.”
A helicopter is called—often unnecessarily.
The patient is admitted to a hospital in Kathmandu.
Guides allegedly induced symptoms using substances like baking soda or excessive medication
Tourists were made to believe they were seriously ill
In extreme cases, this has been described as “manufactured emergencies” (People.com)
Authorities have charged dozens of individuals, including guides and medical personnel, in connection with these activities (The Times of India)
Why This Fraud Was Possible
1. Information Asymmetry
Most trekkers lack medical knowledge and rely heavily on guides for decisions. Fear of altitude sickness makes evacuation an easy choice.
2. High Financial Incentives
A single helicopter rescue can cost thousands of dollars
Insurance companies often cover these costs without immediate verification
3. Remote Geography
No real-time verification in high-altitude zones
Documentation is reviewed only after evacuation
4. Weak Regulation
Despite earlier reforms after a 2018 scandal, enforcement gaps allowed the fraud to continue and expand (Summiters Club)
Impact on Nepal’s Tourism Industry
The consequences extend far beyond financial fraud.
Loss of Trust
International insurers have raised concerns about covering rescues in Nepal, potentially:
Increasing premiums
Limiting coverage
Delaying approvals for genuine emergencies
Risk to Real Patients
If insurers lose confidence:
Legitimate rescue cases may face delays
Life-saving evacuations could become harder to access
Damage to Reputation
Nepal’s global image as a premier trekking destination has been affected, especially during major climbing seasons (The Times of India)
Government Crackdown and Reforms
Authorities, including Nepal Police’s Central Investigation Bureau, have:
Filed organized crime charges
Arrested suspects linked to rescue companies
Investigated hospitals and helicopter operators
Introduced stricter monitoring systems
New measures include:
Better documentation of rescues
Accountability of trekking agencies
Closer scrutiny of insurance claims
Ethical and Medical Perspective
From a medical standpoint, this scandal is deeply concerning.
It exploits genuine fear of altitude illness
It may expose patients to unnecessary evacuation risks
It undermines trust in medical professionals and rescue systems
For healthcare providers and trekkers alike, this raises a critical question:
When is a rescue truly necessary—and who decides?
Conclusion
The Everest rescue insurance fraud reveals a troubling paradox: In a place where helicopters are meant to save lives, they were sometimes used to generate profit.
While the majority of rescues in the Himalayas remain legitimate and life-saving, this scandal highlights the urgent need for:
Stronger regulation
Ethical accountability
Better medical oversight
For Nepal, the challenge now is clear—restore trust in a system where every rescue should mean survival, not exploitation.
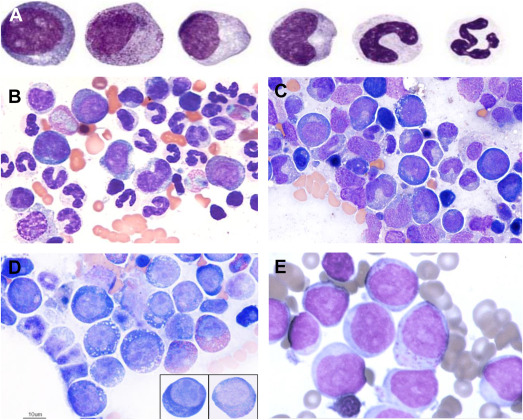
Macrocytic anemia is a hematological condition characterized by the presence of enlarged red blood cells (RBCs), typically reflected by an increased mean corpuscular volume (MCV >100 fL). In pediatric practice, as outlined in Nelson Textbook of Pediatrics, macrocytic anemia represents an important diagnostic category that often signals underlying nutritional deficiencies, bone marrow disorders, or systemic disease.
Classification of Macrocytic Anemia
Macrocytic anemia can broadly be divided into:
Megaloblastic Macrocytic Anemia
Caused by impaired DNA synthesis
Characterized by megaloblasts in the bone marrow
Non-Megaloblastic Macrocytic Anemia
Not associated with defective DNA synthesis
Often due to membrane abnormalities or increased reticulocyte count
Etiology
1. Megaloblastic Causes
Vitamin B12 deficiency
Dietary deficiency (rare in children unless strict vegan diet)
In megaloblastic anemia, impaired DNA synthesis leads to delayed nuclear maturation while cytoplasmic development proceeds normally. This nuclear-cytoplasmic asynchrony results in large, immature erythroid precursors (megaloblasts) and macrocytic RBCs in circulation.
Vitamin B12 and folate are essential cofactors in DNA synthesis. Deficiency of either disrupts thymidine production, impairing cell division.
Clinical Features
Clinical presentation varies depending on severity and cause:
General symptoms
Pallor
Fatigue
weakness
Gastrointestinal
Glossitis (smooth, red tongue)
Poor appetite
Neurological (especially in B12 deficiency)
Paresthesia
Ataxia
Developmental delay (in infants)
Laboratory Findings
Elevated MCV (>100 fL)
Hypersegmented neutrophils (hallmark of megaloblastic anemia)
Low hemoglobin
Peripheral smear: macro-ovalocytes
Serum levels:
↓ Vitamin B12
↓ Folate
Elevated homocysteine (both deficiencies)
Elevated methylmalonic acid (specific for B12 deficiency)
Diagnosis
Diagnosis involves:
Complete blood count (CBC)
Peripheral blood smear
Serum vitamin B12 and folate levels
Bone marrow examination (if unclear or severe cases)
Management
Vitamin B12 Deficiency
Parenteral B12 (cyanocobalamin or hydroxocobalamin)
Lifelong therapy in irreversible causes
Folate Deficiency
Oral folic acid supplementation
Treat underlying cause
⚠️ Important: Always rule out B12 deficiency before treating folate deficiency alone, as folate can worsen neurological symptoms of B12 deficiency.
Macrocytic anemia in children requires a systematic approach to identify underlying causes. As emphasized in Nelson Textbook of Pediatrics, distinguishing between megaloblastic and non-megaloblastic anemia is critical for appropriate management. Early diagnosis and treatment can prevent serious complications, particularly irreversible neurological damage in vitamin B12 deficiency.