Table of Contents
1. Definition
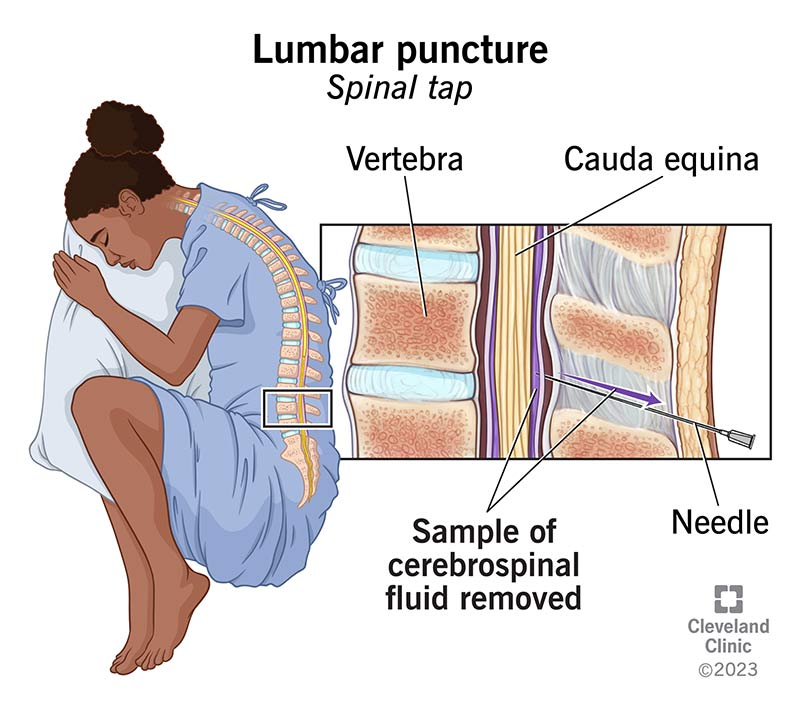
Lumbar puncture (LP) is a procedure in which a needle is inserted into the subarachnoid space of the lumbar spine to obtain cerebrospinal fluid (CSF) for diagnostic or therapeutic purposes.
Commonly done at L3–L4 or L4–L5 intervertebral space.
2. Indications
A. Diagnostic Indications
1. Suspected CNS infection
- Meningitis
- Bacterial
- Viral
- Tubercular
- Fungal
- Encephalitis
- Brain abscess (supportive)
- Neurosyphilis
2. Neonatal sepsis evaluation
Important in:
- Neonates with positive blood culture
- Sepsis with neurologic signs
- Late onset sepsis
- Persistent unexplained illness
3. Neurologic disorders
- Guillain-Barré syndrome (albuminocytologic dissociation)
- Multiple sclerosis
- Demyelinating diseases
- Leukodystrophy
4. Malignancy
- Leukemia CNS involvement
- Lymphoma
- Medulloblastoma spread
5. Subarachnoid hemorrhage
When CT scan is negative but suspicion persists.
B. Therapeutic Indications
- Intrathecal chemotherapy
- Intrathecal antibiotics
- Spinal anesthesia
- CSF pressure reduction (rare)
3. Indications Specific to Neonates
Perform LP in neonates with:
- Suspected meningitis
- Positive blood culture
- Seizures
- Bulging fontanelle
- Apnea / unexplained respiratory deterioration
- Neurological abnormalities
- Late onset sepsis (>72 hrs)
May delay LP in unstable neonate until stabilization.

4. Contraindications
Absolute Contraindications
- Signs of raised intracranial pressure with mass lesion
- Cardiorespiratory instability
- Local infection at puncture site
Relative Contraindications
- Severe thrombocytopenia (<50,000)
- Coagulopathy
- Spinal deformity
- Suspected spinal cord mass
- Severe shock
5. Signs Suggesting Raised ICP (Do NOT perform LP immediately)
- Focal neurological deficits
- Papilledema
- Altered consciousness
- Unequal pupils
- Abnormal posturing
- Hypertension with bradycardia (Cushing triad)
These require neuroimaging first.
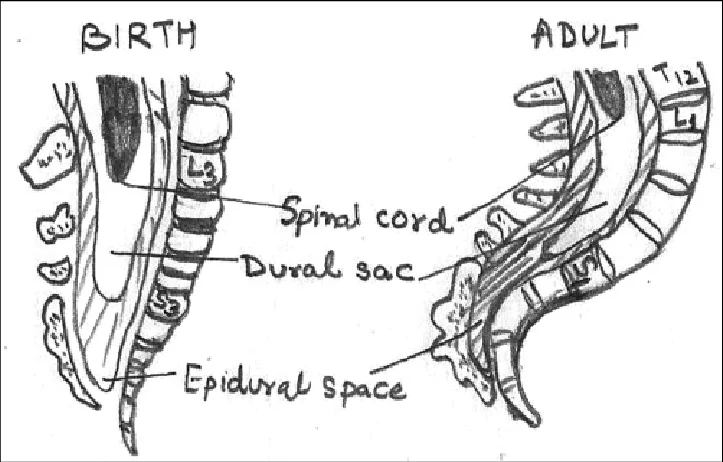
6. Anatomy
LP is done below the conus medullaris.
| Age | Conus level |
|---|---|
| Neonate | L3 |
| Adult | L1–L2 |
Safe spaces:
- L3–L4
- L4–L5
Landmark:
Tuffier line (line joining iliac crests) → L4 vertebra
7. Equipment
- Sterile gloves
- Antiseptic solution
- Sterile drapes
- Spinal needle with stylet
- Manometer
- 3–4 sterile tubes
- Local anesthetic (lidocaine)
- Syringes
- Adhesive dressing
8. Needle Size
| Age | Needle |
|---|---|
| Neonate | 22–25G |
| Infant | 22G |
| Child | 20–22G |
Typical length:
- Neonate: 1.5 inch
- Older children: 2.5 inch
9. Position
1. Lateral decubitus (preferred)
- Knees flexed to chest
- Chin flexed
- Allows opening pressure measurement
2. Sitting position
Used when landmarks difficult.
10. Procedure Steps
- Position child
- Identify L3–L4 or L4–L5
- Clean with antiseptic
- Sterile draping
- Local anesthesia
- Insert needle midline with stylet
- Advance slowly
- Feel “pop” entering subarachnoid space
- Remove stylet → CSF flows
- Collect CSF in tubes
- Replace stylet and remove needle
11. CSF Collection Tubes
| Tube | Test |
|---|---|
| Tube 1 | Biochemistry (protein, glucose) |
| Tube 2 | Microbiology (Gram stain, culture) |
| Tube 3 | Cell count |
| Tube 4 | Special tests (PCR, viral studies) |
12. Opening Pressure
Measured with manometer.
Normal values:
| Age | Pressure |
|---|---|
| Neonates | 2–6 cm H₂O |
| Children | 10–28 cm H₂O |
13. Normal CSF Values
Neonates
| Parameter | Normal |
|---|---|
| Cells | 0–20/mm³ |
| Protein | 40–120 mg/dL |
| Glucose | 2/3 blood glucose |
Infants & Children
| Parameter | Normal |
|---|---|
| Cells | 0–5/mm³ |
| Protein | 15–45 mg/dL |
| Glucose | 2/3 serum |
14. CSF Interpretation
Bacterial Meningitis
| Finding | Result |
|---|---|
| Cells | ↑ (100–10,000) |
| Cell type | Neutrophils |
| Protein | ↑↑ |
| Glucose | ↓ |
| Opening pressure | ↑ |
Viral Meningitis
| Finding | Result |
|---|---|
| Cells | 10–1000 |
| Cell type | Lymphocytes |
| Protein | Mild ↑ |
| Glucose | Normal |
TB Meningitis
| Finding | Result |
|---|---|
| Cells | 50–500 |
| Type | Lymphocytes |
| Protein | ↑↑ |
| Glucose | ↓ |
15. Complications
Immediate
- Traumatic tap
- Pain
- Bleeding
- Infection
Post LP
- Post-LP headache
- Back pain
Serious
- Brain herniation
- Epidural hematoma
- Nerve injury
16. Traumatic Tap Differentiation
| Feature | Traumatic tap | SAH |
|---|---|---|
| RBC count | Decreases in later tubes | Same in all tubes |
| Clot | Present | Absent |
| Xanthochromia | Absent | Present |
17. Reasons for Failed LP
- Wrong level
- Poor positioning
- Obesity
- Dehydration
- Needle obstruction
18. When NOT to Delay Antibiotics
In suspected meningitis:
- Start antibiotics immediately
- LP should not delay treatment
19. Special Considerations in Neonates
- Higher CSF protein normally
- CSF WBC slightly higher
- LP often required in late onset sepsis
- May be delayed if unstable
✅ Exam Pearls (Important for MD / Residency)
- Best site: L3–L4
- Neonatal normal CSF protein higher
- Always replace stylet before removing needle
- Opening pressure measured only in lateral position
- Papilledema → neuroimaging before LP