
Table of Contents
Prolonged PT/INR in neonates usually reflects abnormalities in the extrinsic and common coagulation pathways (Factors I, II, V, VII, X).
The causes can be grouped into physiologic, nutritional, hepatic, consumptive, inherited, and iatrogenic causes.
1. Physiological Causes
Physiologic immaturity of coagulation system
- Normal neonates (especially preterms) have:
- Lower vitamin K–dependent clotting factors
- Reduced hepatic synthesis
- Mild PT prolongation may occur in:
- Prematurity
- Very low birth weight infants
2. Vitamin K Deficiency (Most Important Cause)
Vitamin K Deficiency Bleeding (VKDB)
Most common clinically important cause of prolonged PT in neonates.

Why PT increases first?
Factor VII has the shortest half-life → PT prolongs earliest.
Risk factors
- No vitamin K prophylaxis at birth
- Exclusive breastfeeding
- Maternal anticonvulsants:
- Phenytoin
- Phenobarbital
- Carbamazepine
- Maternal anti-TB drugs:
- Rifampicin
- Isoniazid
- Malabsorption/cholestasis
- Prolonged antibiotics
Types
| Type | Timing |
|---|---|
| Early VKDB | <24 hr |
| Classical VKDB | Day 2–7 |
| Late VKDB | 2 weeks–6 months |
Labs
- ↑ PT/INR (earliest finding)
- Later ↑ aPTT
- Normal platelets initially
- Rapid correction after vitamin K
3. Liver Disease / Hepatic Dysfunction
Neonatal liver dysfunction reduces clotting factor synthesis.
Causes
- Neonatal hepatitis
- Biliary atresia
- Cholestatic liver disease
- Sepsis-associated liver dysfunction
- Hypoxic ischemic injury
- Metabolic liver disease
- Galactosemia
- Tyrosinemia
Labs
- ↑ PT/INR
- May not correct with vitamin K if severe hepatocellular failure
4. Disseminated Intravascular Coagulation (DIC)
Consumptive coagulopathy causing depletion of clotting factors.
Common neonatal triggers
- Sepsis
- Birth asphyxia
- NEC
- Shock
- Severe hypoxia
- Meconium aspiration
- Severe hemolysis
Labs
- ↑ PT
- ↑ aPTT
- ↓ fibrinogen
- ↓ platelets
- ↑ D-dimer/FDP
5. Sepsis
Can prolong PT due to:
- Hepatic dysfunction
- DIC
- Cytokine-mediated coagulopathy
- Vitamin K deficiency from poor feeding/antibiotics

6. Congenital Coagulation Factor Deficiencies
Factor VII deficiency
- Isolated prolonged PT
- Normal aPTT
Deficiencies affecting common pathway
- Factor II deficiency
- Factor V deficiency
- Factor X deficiency
- Fibrinogen disorders
Clues
- Family history
- Bleeding despite vitamin K
- Persistent abnormal PT
7. Massive Bleeding / Dilutional Coagulopathy
Occurs after:
- Massive transfusion
- Exchange transfusion
- Severe hemorrhage
Mechanism:
- Dilution of clotting factors
8. Anticoagulant Exposure
Maternal drug exposure
- Warfarin
- Anticonvulsants
- Anti-TB drugs
Neonatal medications
- Heparin contamination of sample (usually affects aPTT more)
9. Cholestasis / Fat Malabsorption
Leads to poor vitamin K absorption.
Causes
- Biliary atresia
- Neonatal cholestasis
- Cystic fibrosis
- Intestinal disease
10. Laboratory / Sampling Errors
Always exclude before extensive workup.
Causes
- Underfilled citrate tube
- Clotted sample
- Heparin contamination
- Difficult sampling
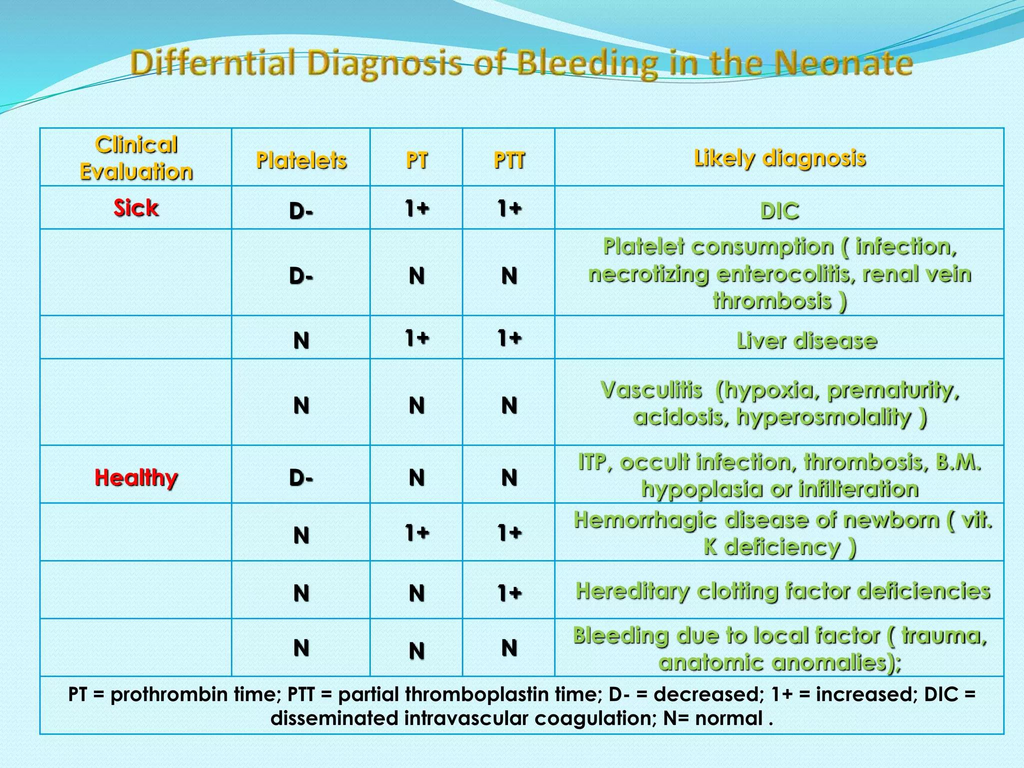
Important High-Yield Pattern Recognition
| Pattern | Likely Cause |
|---|---|
| Isolated ↑ PT | Vitamin K deficiency, Factor VII deficiency |
| ↑ PT + ↑ aPTT | Liver disease, DIC, severe VKDB |
| ↑ PT + thrombocytopenia | DIC, sepsis |
| PT corrects after vitamin K | VKDB |
| PT not correcting with vitamin K | Liver failure or factor deficiency |
High-Yield Neonatal Causes to Remember
- Vitamin K deficiency
- Sepsis
- DIC
- Liver disease/cholestasis
- Prematurity
- Congenital factor deficiency
- Maternal drug exposure
🚨 Increased PT/INR in Neonates — High Yield NICU Causes
🩸 Common causes of prolonged PT/INR in newborns:
▪️Vitamin K deficiency (most common)
▪️Sepsis
▪️DIC
▪️Liver disease / cholestasis
▪️Prematurity (physiologic immaturity)
▪️Congenital factor deficiencies (especially Factor VII)
▪️Maternal drugs
• Anticonvulsants
• Anti-TB drugs
• Warfarin
▪️Massive bleeding / dilutional coagulopathy
▪️Laboratory sampling errors
⚡ High-yield tip:
➡️ PT rises EARLY in vitamin K deficiency because Factor VII has the shortest half-life.
🧠 Pattern to remember:
🔹 Isolated ↑ PT → Vitamin K deficiency / Factor VII deficiency
🔹 ↑ PT + ↑ aPTT → DIC or liver disease
🔹 Corrects after vitamin K → VKDB likely
PT/INR evaluates the extrinsic coagulation pathway and is commonly used in neonatal coagulation assessment. (bmcpediatr.biomedcentral.com)