Table of Contents
Macrocytic anemia is a hematological condition characterized by the presence of enlarged red blood cells (RBCs), typically reflected by an increased mean corpuscular volume (MCV >100 fL). In pediatric practice, as outlined in Nelson Textbook of Pediatrics, macrocytic anemia represents an important diagnostic category that often signals underlying nutritional deficiencies, bone marrow disorders, or systemic disease.
Classification of Macrocytic Anemia
Macrocytic anemia can broadly be divided into:
- Megaloblastic Macrocytic Anemia
- Caused by impaired DNA synthesis
- Characterized by megaloblasts in the bone marrow
- Non-Megaloblastic Macrocytic Anemia
- Not associated with defective DNA synthesis
- Often due to membrane abnormalities or increased reticulocyte count
Etiology
1. Megaloblastic Causes
- Vitamin B12 deficiency
- Dietary deficiency (rare in children unless strict vegan diet)
- Malabsorption (e.g., pernicious anemia, ileal disease)
- Folate deficiency
- Poor dietary intake
- Increased requirement (e.g., infancy, hemolytic anemia)
- Malabsorption syndromes
2. Non-Megaloblastic Causes
- Liver disease
- Hypothyroidism
- Reticulocytosis (e.g., hemolysis, blood loss)
- Bone marrow disorders (e.g., aplastic anemia, myelodysplasia)
- Drug-induced (e.g., anticonvulsants, chemotherapy)
Pathophysiology
In megaloblastic anemia, impaired DNA synthesis leads to delayed nuclear maturation while cytoplasmic development proceeds normally. This nuclear-cytoplasmic asynchrony results in large, immature erythroid precursors (megaloblasts) and macrocytic RBCs in circulation.
Vitamin B12 and folate are essential cofactors in DNA synthesis. Deficiency of either disrupts thymidine production, impairing cell division.
Clinical Features
Clinical presentation varies depending on severity and cause:
- General symptoms
- Pallor
- Fatigue
- weakness
- Gastrointestinal
- Glossitis (smooth, red tongue)
- Poor appetite
- Neurological (especially in B12 deficiency)
- Paresthesia
- Ataxia
- Developmental delay (in infants)
Laboratory Findings
- Elevated MCV (>100 fL)
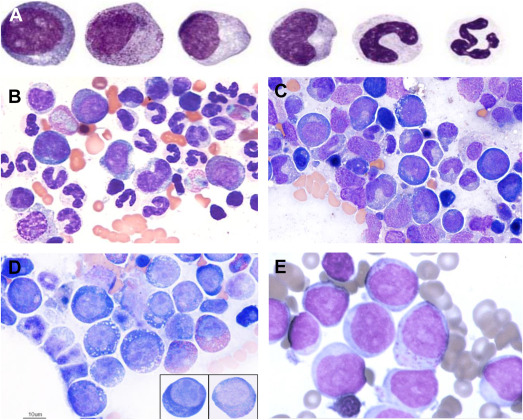
- Hypersegmented neutrophils (hallmark of megaloblastic anemia)
- Low hemoglobin
- Peripheral smear: macro-ovalocytes
- Serum levels:
- ↓ Vitamin B12
- ↓ Folate
- Elevated homocysteine (both deficiencies)
- Elevated methylmalonic acid (specific for B12 deficiency)
Diagnosis
Diagnosis involves:
- Complete blood count (CBC)
- Peripheral blood smear
- Serum vitamin B12 and folate levels
- Bone marrow examination (if unclear or severe cases)
Management
Vitamin B12 Deficiency
- Parenteral B12 (cyanocobalamin or hydroxocobalamin)
- Lifelong therapy in irreversible causes
Folate Deficiency
- Oral folic acid supplementation
- Treat underlying cause
⚠️ Important: Always rule out B12 deficiency before treating folate deficiency alone, as folate can worsen neurological symptoms of B12 deficiency.
Complications
- Neurological deficits (irreversible if untreated)
- Growth retardation in children
- Increased risk of infections due to pancytopenia
Prevention
- Adequate dietary intake (green leafy vegetables, animal products)
- Supplementation in high-risk groups
- Early detection in infants and children
Conclusion
Macrocytic anemia in children requires a systematic approach to identify underlying causes. As emphasized in Nelson Textbook of Pediatrics, distinguishing between megaloblastic and non-megaloblastic anemia is critical for appropriate management. Early diagnosis and treatment can prevent serious complications, particularly irreversible neurological damage in vitamin B12 deficiency.