Table of Contents
The anterior fontanelle is the largest fontanelle of the newborn skull and normally remains open during early infancy to allow brain growth and skull expansion.
1. Normal Anatomy and Physiology
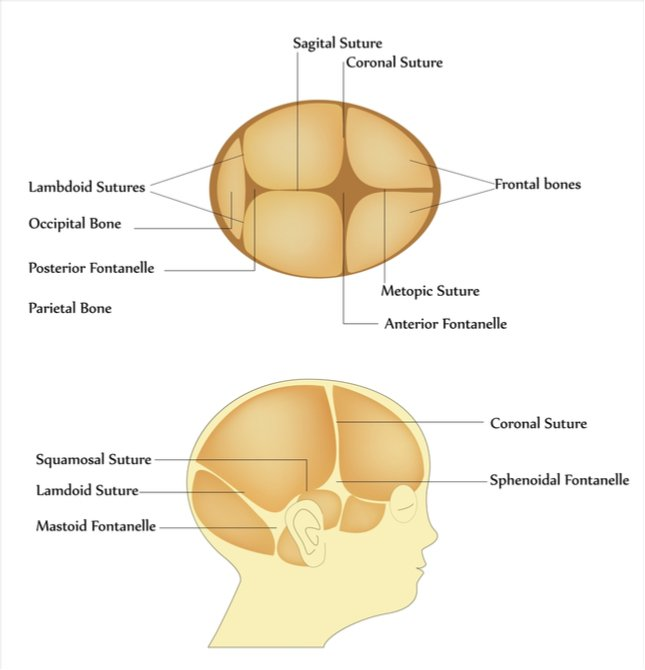
- The anterior fontanelle lies at the junction of:
- Two frontal bones
- Two parietal bones
- Shape: Diamond-shaped
- Average size at birth: 1–4 cm
- Normal closure: 9–18 months
Functions:
- Allows rapid brain growth
- Facilitates molding during vaginal delivery
- Serves as a clinical window for intracranial pressure assessment
When the Anterior Fontanelle Is Absent at Birth
A non-palpable or absent anterior fontanelle suggests premature fusion of cranial sutures or abnormal skull ossification.
This finding must always be evaluated carefully because it may indicate craniosynostosis or underlying pathology.
Causes of Absent Anterior Fontanelle
1. Craniosynostosis (Most Important Cause)
Premature fusion of one or more cranial sutures prevents normal skull expansion.
Types include:
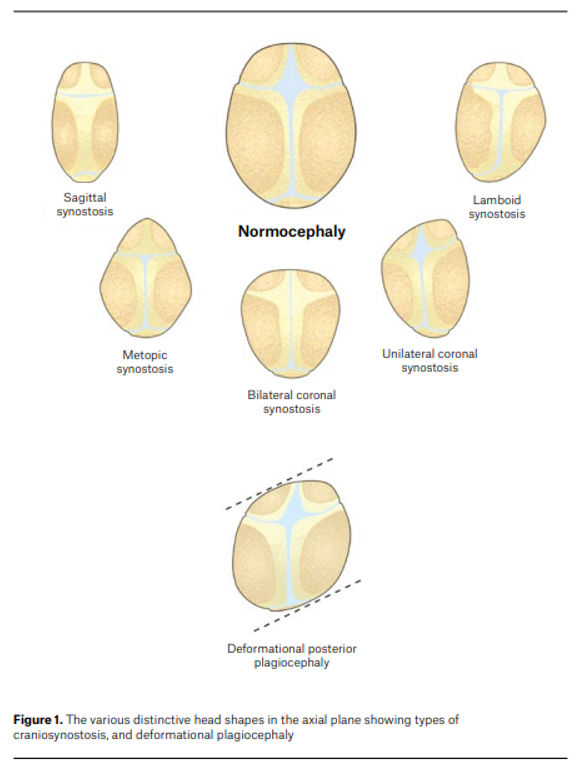
| Suture involved | Resulting head shape |
|---|---|
| Sagittal | Scaphocephaly (long narrow skull) |
| Coronal | Brachycephaly |
| Metopic | Trigonocephaly |
| Multiple sutures | Oxycephaly |
Consequences:
- Restricted skull growth
- Raised intracranial pressure
- Neurodevelopmental impairment if untreated
2. Hyperthyroidism (Congenital Thyrotoxicosis)
Seen in infants of mothers with Graves disease
Mechanism:
- Increased thyroid hormone → accelerated bone maturation
- Leads to early closure of sutures and fontanelles
Associated features:
- Irritability
- Tachycardia
- Poor weight gain
- Goiter
- Exophthalmos (rare in neonates)
3. Microcephaly
Brain growth failure leads to small skull size, so sutures close early.
Common causes:
- Intrauterine infections (TORCH)
- Genetic syndromes
- Severe hypoxic injury
- Metabolic disorders
4. Skeletal Dysplasias
Some bone disorders cause abnormal skull ossification.
Examples:
- Osteopetrosis
- Thanatophoric dysplasia
5. Normal Variant
Rarely the fontanelle is very small or difficult to palpate, but sutures remain open and skull growth is normal.
Clinical Evaluation
1. History
Ask about:
Maternal history
- Hyperthyroidism
- Antithyroid drugs
- TORCH infections
Perinatal history
- Birth trauma
- Neonatal illness
Family history
- Craniosynostosis
- Genetic syndromes
Developmental history
- Feeding difficulty
- Poor growth
- Developmental delay
2. Physical Examination
Head Examination
Assess:
| Feature | Significance |
|---|---|
| Head circumference | Detect microcephaly |
| Skull shape | Suggest specific craniosynostosis |
| Palpation of sutures | Check if fused or ridged |
| Remaining fontanelles | Posterior fontanelle status |
Look for Associated Signs
Neurologic:
- Irritability
- Vomiting
- Bulging veins
Systemic:
- Signs of hyperthyroidism
- Dysmorphic features
Investigations
1. Imaging
Skull X-ray
- Shows fused sutures
Cranial ultrasound
- If some fontanelle is open
CT scan with 3D reconstruction
- Gold standard for diagnosing craniosynostosis
2. Laboratory Tests
If systemic cause suspected:
| Test | Purpose |
|---|---|
| Thyroid function test | Detect neonatal thyrotoxicosis |
| TORCH screening | If infection suspected |
| Genetic testing | Syndromic craniosynostosis |
Complications
If due to craniosynostosis:
- Raised intracranial pressure
- Visual impairment
- Developmental delay
- Cognitive impairment
Management
1. Craniosynostosis
Referral to pediatric neurosurgery
Treatment:
- Surgical cranial vault remodeling
- Usually performed within first year of life
2. Neonatal Hyperthyroidism
Treat underlying condition:
- Antithyroid drugs
- Beta-blockers
3. Microcephaly
Management depends on cause:
- Developmental support
- Treat underlying infection/metabolic disease
Clinical Pearls (High-Yield)
- Anterior fontanelle absent at birth → think craniosynostosis first.
- Always measure head circumference.
- Check skull shape and sutures carefully.
- 3D CT scan confirms diagnosis.
- Early surgical correction prevents intracranial hypertension and neurodevelopmental damage.